Conditions
A structured, family-friendly guide to pediatric heart conditions.
Select a condition
Choose a condition from the left to view the full guide.
Visual Heart Flow Library
Simple hand-drawn flow diagrams to support family discussions with your pediatric cardiologist.
Ventricular septal defect (VSD)
A VSD is a hole in the wall that separates the ventricles or the lower chambers of the heart. A VSD may occur in isolation or along with other defects in the heart. What happens to the baby then depends on the vsd AND the associated defects. This post deals with an isolated VSD. It is a congenital heart defect that is present at birth. Over time, in some babies, this hole closes by itself. Once a VSD is closed (by itself or with surgery), the baby has a totally normal life like any other child.
Symptoms of VSD
- Large sized VSD: The affected baby will not have any issues for the first month of life. Slowly, the mother will notice that her baby tires out while breast feeding: as if catching their breath while running, sweating and pausing between swallowing. The weight of the baby will not rise like it is supposed to. The baby will get frequent cough/cold/chest infections. Mothers complain that a doctor’s visit is needed every week!
- Small sized VSD: The affected baby is unlikely to have any symptoms from the VSD. However even a small vsd can develop complications hence regular follow up at the pediatric cardiac OPD is essential.
- Moderate sized VSD: the affected baby has some symptoms of the large vsd but not of that severity.
- Older child with a large uncorrected VSD and pulmonary hypertension: this is a special group. Such a child/adult who has not been operated upon, will have tiredness with exertion. The nails may be curvy (clubbing) and have a bluish tinge.
Causes of VSD
A VSD is a developmental disorder present at birth. What exactly causes it is not very clear. There are certain factors affecting mothers during pregnancy that increase the risk of VSD and other heart defects in babies. Some of the known risk factors are family history of heart defects, mother on certain medications in early pregnancy, diabetes in mother from early pregnancy, IVF pregnancy, anomaly scan showing a defect in any other organ system of the fetus (brain, gut, kidney etc).
How blood flows in a heart with a VSD
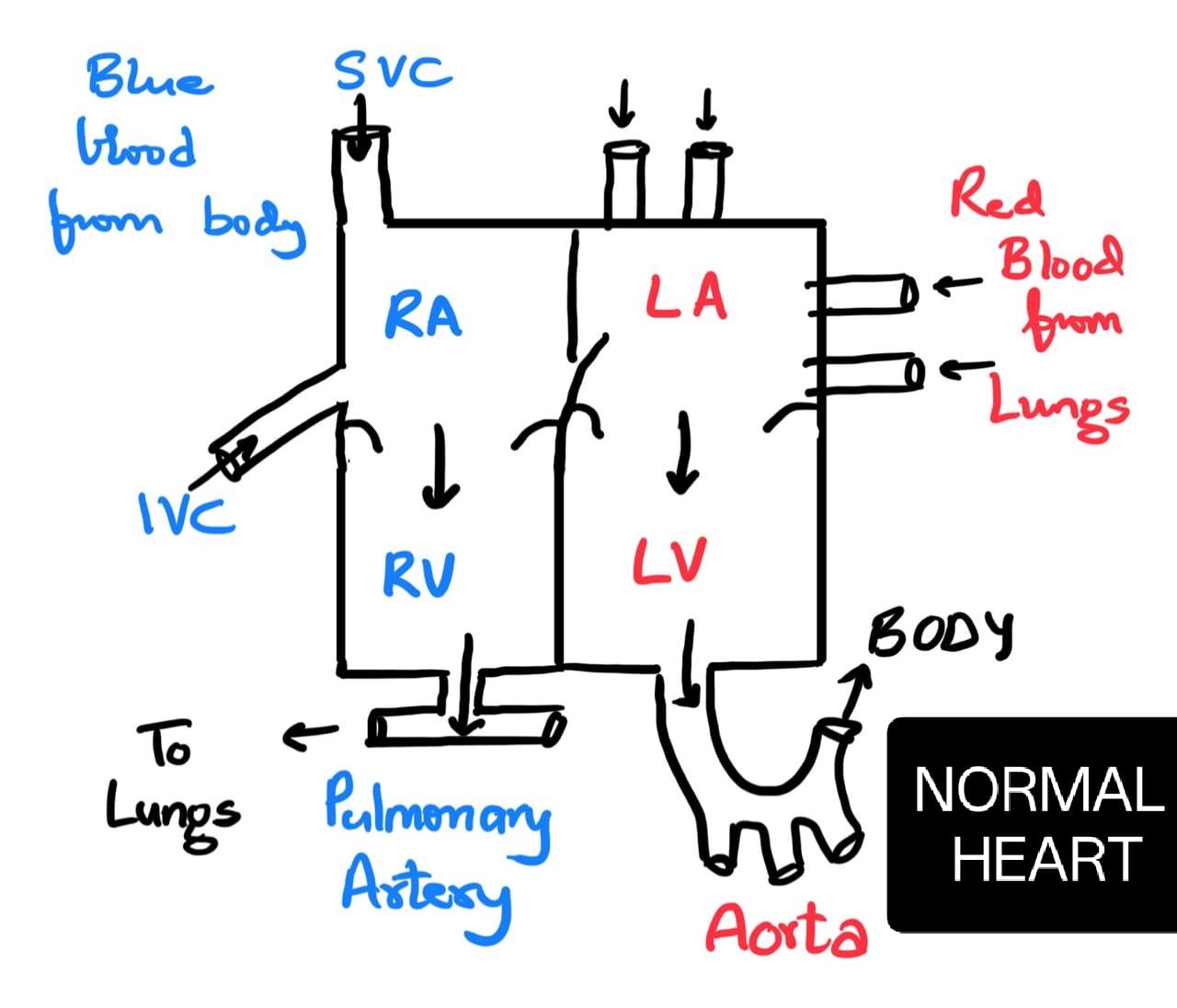
- To understand VSD better, it is important to know how the normal heart works.
- The left heart has 2 chambers and the right heart has 2 chambers.
- The top 2 chambers (RA and LA) are the collecting chambers while the bottom 2 chambers (RV and LV) are pumping chambers.
- Pure blood is pumped by the LV to the whole body. The body’s organs uses the oxygen in that blood and makes the blood impure.
- The impure blood returns to the RA and is pumped by the RV to the lungs.
- When we breathe, the oxygen in our breath enters the blood and makes it pure again. The pure blood enters LA and is pumped out to the body by the LV.
- Thus the heart supports 2 circuits.
- The left circuit pumps pure blood to the body and the right circuit pumps impure blood to the lungs.
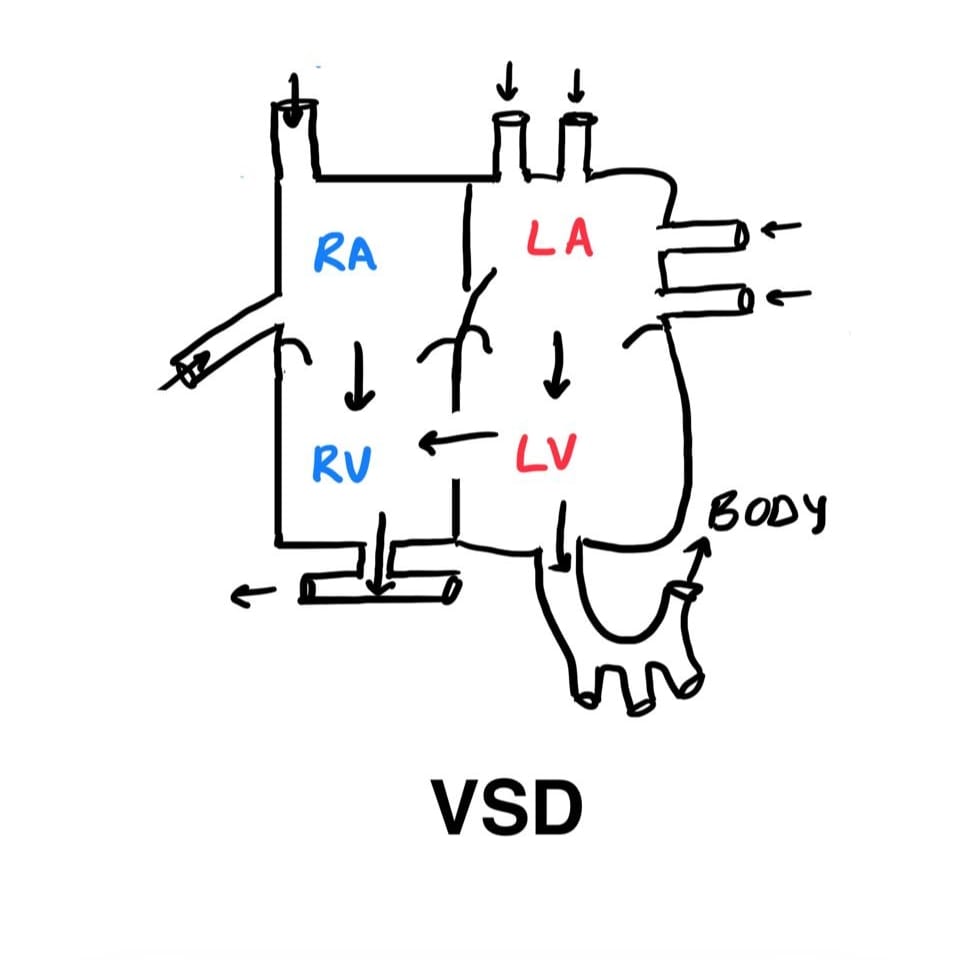
- In a child with a VSD, the wall (SEPTUM) between the LV and the RV has a hole in it.
- So blood flows from the LV to the RV and then to the lungs.
- This means extra blood ends up going to the lungs. The congested lungs get infected relatively easily.
- Also, the LA and LV become bigger in size and pressure in the lung arteries also rises (pulmonary hypertension).
Types of VSDs
- Perimembranous VSD: It is the most common type. It can close on its own if small or medium sized. Only a pediatric cardiac specialist can tell if it may close and if it is safe to wait for its spontaneous closure.
- Muscular VSD: This type is also very common. This type of defect has the best chance of closing on its own.
- Inlet Ventricular Septal Defect: this type is relatively rare. It does not close on its own and requires surgical closure.
VSDs can also be classified based on the size. However, no matter what the size or where it is located, all babies/children with VSDs need to have regular follow up visits in a pediatric cardiac OPD.
Complications of VSD
- Pulmonary hypertension: this means that the pressure in the lung arteries is high. This returns to normal once the VSD is closed, provided the vsd is closed at the correct time. If the VSD remains uncorrected for a long time, the pulmonary hypertension may become permanent. This has devastating consequences of quality and quantity of life.
- Bacterial Endocarditis: This is a rare complication seen in uncorrected vsds, no matter how big or small they may be. It is a potentially life threatening infection of the inside lining of the heart.
- Aortic valve prolapse: When a VSD borders the aortic valve frame, the circular frame of the valve gets stretched and the valve leaflets suspended from it, don’t get enough support. Eventually, the valve leaks (also called aortic regurgitation) and this can become a bigger problem than the VSD itself. Surgery involves closing the vsd. If the valve is too damaged, it needs to be repaired or replaced (rarely).
- DCRV: this stands for double chamber right ventricle. This complication is seen in tiny or small VSDs. Extra muscle bundles form in the RV and prevent normal flow of blood out of the RV. An affected child becomes tired with playing. Surgery involves closing the VSD and cutting the extra muscle bundles. This complication is completely treatable.
Diagnosis
Hearing an abnormal heart murmur while listening to the heart sounds with a stethoscope will raise a suspicion of a VSD. The paediatrician may also suspect a VSD if a baby gets tired with breast feeding, fails to gain weight adequately or get repeated chest infections.
The diagnosis is confirmed by an Echocardiogram- In this test, the doctor uses ultra-sound waves to assess the heart function as well as the blood flow. It helps to determine the size and location of the VSD and also other technical details that help the doctor decide the plan of action ahead.
- Pulse oximetry
- ECG
- Cardiac catheterization
VSD repair – When to do
- Large VSD: A large VSD is closed by surgery at age 3 months. This is because at 3 months, the risk/benefit ratio is in favour of the infant getting operated. Even more major heart defects are closed at birth or by 1 month but that decision is taken because it is not in the baby’s interest to wait any longer. On the other hand, waiting for more than 3months of age to close a VSD may hamper a baby’s growth and make him/her susceptible to chest infections.
- Small or moderate sized VSD: A child with such a VSD is kept under careful follow up by the pediatric cardiologist. The VSD needs to be closed if any complication develops.
VSD treatment
The standard treatment for a VSD is to close it surgically. An open heart surgery can be safely performed in most dedicated pediatric cardiac centres, in this day and age. The duration of the surgery is around 3-4 hours. The baby will be in an ICCU for 2-3days after surgery. The average stay in the hospital will be for 6-7days.
Another way to close certain VSDs, especially muscular ones, is by a non surgical method. This is carried out by the interventional pediatric cardiologist in the cardiac catheterization laboratory. An umbrella device is placed across the vsd to plug it. The device is introduced through the groin vessel. There is no cut/suture in this procedure. The patient gets to go home the next day. Only certain kinds of VSDs can be closed by this method. The pediatric cardiologist can determine whether the VSD is suitable for device closure after a detailed echocardiogram.
A child with a successfully closed VSD can perform all routines of any other child including performing well in academics, sports etc. There are no restrictions placed.
Spontaneous closure and surgery
Some defects close by itself without any treatment after a while (usually before two years of age). If the VSD is large and remains open, a repair surgery will be necessary to close the hole. A VSD repair is either a cardiac catheterization procedure or an open-heart surgery. In cardiac catheterization, the surgeon will repair the hole with a patch by passing it through a large vein in the groin. Large VSDs will need open-heart surgery, to place the patch.
Tetralogy of Fallot (TOF)
TOF is a major congenital heart defect consisting of four abnormalities. It leads to a bluish tinge (cyanosis) of the lips and nails, especially when walking or crying. The defect worsens with time and needs surgical correction ideally between 6 months and 1 year of age. Children do very well after repair, with good quality and quantity of life.
Causes of TOF
TOF is a developmental defect present at birth. Its exact cause is unknown, but several maternal risk factors increase its likelihood: family history of heart defects, maternal diabetes, IVF pregnancy, and medications in early pregnancy. Around 30–40% of children with TOF have chromosomal abnormalities like 22q11 deletion, which may also cause cleft palate, immunity issues, developmental delay, and calcium problems.
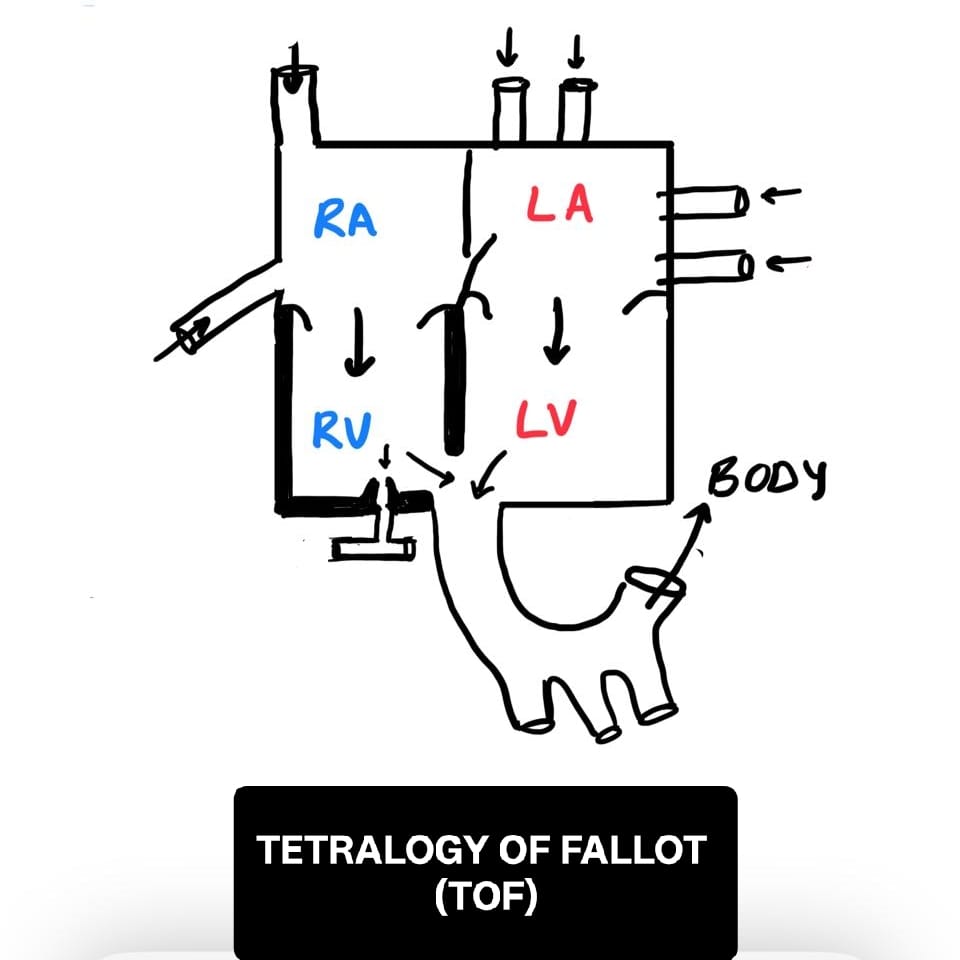
What are the 4 defects in TOF?
- Ventricular Septal Defect (VSD): Hole between the lower chambers.
- Pulmonary stenosis: Narrowing at the RV exit and pulmonary valve.
- Overriding aorta: Aorta arises from both the LV and RV.
- Right ventricular hypertrophy: Thickened right ventricle muscle.
How blood flows in a heart with TOF
Normally, pure blood is pumped to the body by the LV and impure blood is pumped to the lungs by the RV. In TOF, due to pulmonary stenosis, blood from the RV flows through the VSD into the aorta, mixing impure and pure blood. This reduces oxygen levels in the body and causes cyanosis. The narrowing and structural changes disrupt normal circulation.
Symptoms of TOF
- Bluish discoloration (cyanosis) of skin, lips, and nails
- Rapid or difficult breathing
- Extreme tiredness with mild activity
- Fainting, irritability, or crying spells
- Bulbous (clubbed) fingers and toes
- Tendency to squat during play (to ease breathing)
- "Tet spells" – sudden bluish discoloration due to low oxygen levels, often triggered by crying or feeding
- Heart murmur detected during examination
Diagnosis of TOF
The primary tool for diagnosis is an echocardiogram. Additional tests may include ECG, CT scan, cardiac catheterization, and genetic testing (FISH for 22q11 deletion).
TOF repair – When to do
- Ideal time: Between 4–6 months of age, based on clinical and echocardiographic findings.
- BT Shunt: If the baby is very ill or has small pulmonary arteries, a temporary bypass surgery (BT shunt) is done first. Complete repair follows later.
Treatment of TOF
TOF is corrected through surgery. Total correction (intracardiac repair) involves closing the VSD and relieving the pulmonary stenosis. The surgery takes around 4–5 hours, with 2–3 days in the ICU. Some babies may require an earlier BT shunt. Lifelong follow-up is essential.
Complications of untreated TOF
- Death or brain damage due to cyanotic spells
- Strokes from blood clots reaching the brain
- Bleeding in lungs
- Bacterial endocarditis (infection of the heart lining)
- Thickened blood leading to headaches, dehydration, gout
- Irregular heart rhythms (e.g., atrial fibrillation)
- Heart failure
Prognosis and follow-up
After successful surgery, children with TOF can live normal lives, including school and sports. Lifelong monitoring with ECG, echocardiography, and stress tests is required. Rarely, some children may need further procedures due to valve leaks or arrhythmias.
Pulmonary Hypertension (PH)
Pulmonary hypertension (PH) is a condition where the lung artery pressure is abnormally high. The normal lung artery pressure is 1/4th or less of the BP that is measured in our arm.
Severe PH is harmful for health. It prevents the affected person from responding to exercise or exertion in a normal manner. So, the person gets tired very soon and may faint or the body may show swelling. If treatment is not started, it can be life threatening.
PH can be due to a problem in the heart or lungs or sometimes in the blood vessels. An example is a large hole in the heart (VSD) that causes PH. The PH disappears once the VSD is closed. In such cases, the child has symptoms of the VSD.
Occasionally, the PH is Primary; that means there is no other detectable reason for the PH, that can be treated and then one can hope that the PH will disappear.
This kind of primary PH is dangerous for health. It needs aggressive treatment. This treatment starts with medicines. When medicines don’t help, other measures have to be taken. These include surgeries which could help with symptoms (Pott’s shunt) or, ultimately, heart-lung transplant surgery.
This article is about the condition where there is PH but there is no identifiable reason for the PH. For the sake of simplicity, this will be referred to as primary PH for the rest of the article.
Causes of Primary PH
A lot of investigations are performed in any child who has PH. The aim to make sure to diagnose ANY cause for the PH so that treatment for the cause can be done. These investigations include blood tests, CT scans, MRI, echocardiography, sleep studies, cardiac catheterization and genetic studies.
If nothing is found in these studies, then the child is assumed to have primary PH. Some situations predispose to developing primary PH. Like birth prematurity, exposure to certain pollutants or drugs, being overweight and having other people in the family with PH. Researchers have found abnormal structure of the lung vessels in patients with primary PH. But overall, it is a poorly understood entity.
How the heart and lungs are affected in primary PH
To understand primary PH better, it is important to know how the normal heart works. The left heart has 2 chambers and the right heart has 2 chambers. The top 2 chambers (RA and LA) are the collecting chambers while the bottom 2 chambers (RV and LV) are pumping chambers. Pure blood is pumped by the LV to the whole body. The body’s organs (brain, gut, muscles etc) use the oxygen in that blood and makes the blood impure. The impure blood returns to the RA and is pumped by the RV to the lungs. When we breathe, the oxygen in our breath enters the blood and makes it pure again. The pure blood enters LA and is pumped out to the body by the LV.
Thus, the heart supports 2 circuits. The left circuit pumps pure blood to the body and the right circuit pumps impure blood to the lungs. The left circuit works at a high pressure (the BP measured in the arm) while the right circuit works at a low pressure (pulmonary pressure).
When primary PH develops, the right side of the heart suffers first. The RV walls become thick, the walls of the lung arteries (pulmonary arteries) also become thickened. Over time, the thickened RV fails, first with exercise and then even at rest and heart failure results. The thickened lung arteries become prone to blood clots inside them. Ultimately the left side of the heart also suffers and its function is also affected.
Complications of PH
- Enlargement of the right side of the heart
- Right-sided heart failure
- Clots in the heart, lung vessels
- Left-sided heart failure
Symptoms of PH
- Sudden Fainting spells
- Getting tired with any exertion
- Swelling in the legs, tummy, face
- Younger children and babies may just show failure to gain weight and fast breathing rate.
PH diagnosis
In a child with a doubt of PH, the doctor will advise the following tests:
- Echocardiogram: This is sonography of the heart. It is not 100% accurate to pick up PH. But is 100% required when PH is suspected because it may reveal the cause of the PH to be in the heart! In addition, the effect of PH on the heart will be seen on the echo. So, this test may be repeated many times.
- ECG: This is an important screening test that gives information on the heart rate and the rhythm.
- Cardiac catheterization: This is very sensitive and accurate to diagnose PH. It involves placing long thin tubes (catheters) from the groin vessels, to the heart and the lung arteries. The pressure in the right heart can be directly measured this way. In addition, other numbers (CO, PVR etc) can be calculated from the pressure. These numbers are important to understand the PH better. This test is done in the Cardiac Cath Lab. The child has to be relatively healthy to undergo this test. If the child is very sick, the child maybe admitted, treated with oxygen, intravenous or inhaled medicines and then taken for the cardiac Cath test. This test may also be repeated every 2-3 years.
- Scans like Chest Xray, CT scan or MRI: These are a must to investigate the cause of the PH. These will also help the doctor team understand the primary PH better and adjust medicines accordingly.
- Blood tests: These are essential to investigate the cause of PH. There are also markers of heart failure like blood BNP and NT pro BNP levels that go up and down depending on degree of heart failure.
- 6-minute walk test: The older child is made to walk for 6minutes. The result of the test is used to guide the treatment of PH. It will be repeated every 6months.
Treatment of PH
It cannot be stressed enough: it is vital to find the cause of the PH if any. If a treatable condition is found, the PH is easier to manage. This paragraph is about treating PH when there is no underlying condition causing it.
Medicines: tablets (syrups) can be started to control the PH. Generally, one medicine is started, and another added if the response is not satisfactory. There are also medicines that can be given via nose (inhaled), through an IV line or under the skin (subcutaneous). The major effect of these medicines is to keep the PH under control. There are many medicines available. They differ in how they keep the PH under control. Some examples are sildenafil, tadalafil, bosentan, ambrisentan, macitentan, triprostinil, iloprost and riociguat. Some medicines are not freely available.
Advanced options
Atrial Septostomy: The thin wall between the 2 upper chambers of the heart is punctured and a hole is made. This hole acts like a pop off for high pressure to vent from the right heart to the left. A pediatric lung/heart specialist can best guide you on whether this is a right option for your child.
Pott’s shunt: A small tube is placed between the left and the right hearts at the level of the Arteries that come out from the left and right hearts. This tube can vent the pressure of the right heart artery (pulmonary artery) into the left heart artery (aorta) when the PH is very high. A pediatric lung/heart specialist can best guide you on whether this is a right option for your child. A Pott’s shunt is not the cure for your child’s PH. However, it may be the only option for your child if he/she continues to have symptoms despite taking medicines and is waiting for a heart-lung transplant. Most experts feel that a Pott’s shunt is a better option than atrial septostomy.
Heart-Lung transplant: A brain dead donor’s heart+lungs are placed in the chest, and the diseased heart/lungs are removed. This is a major surgery and is the beginning of lifelong care and medicines. At the present time, the long-term results of heart-lung transplants are not very encouraging. However, it may be the only option for some patients and may be lifesaving. It cannot be done “ on demand”, unlike Pott’s shunt. There is a detailed procedure involving local government office and rules. The patient is “listed” for the transplant and then remains on the “waiting list” till a suitable donor is found.
Pott’s surgery – When to do
In a child with primary PH, the physician team will look into the following aspects:
- Are the medicines optimized? If not, adjustments will be made
- The severity of symptoms? Is the child unable to walk/run? Does he/she get fainting spells?
- How is the echocardiogram? What is the status of the RV?
It is important to do the Pott’s shunt at the right time. Too early or too late are both undesirable.
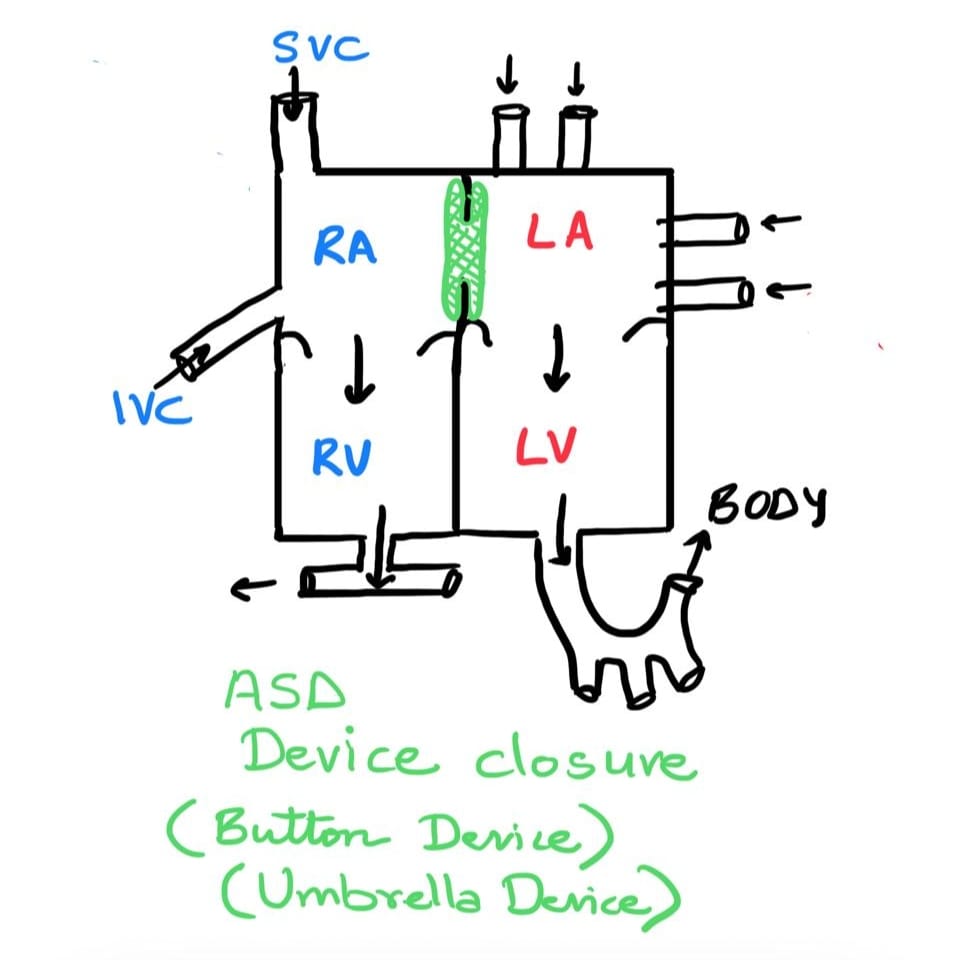
Atrial Septal Defects (ASD)
An atrial septal defect is a hole in the wall that separates the atria or the upper chambers of the heart.
It is a congenital heart defect that is present at birth. Over time, in some babies, this hole closes by itself.
An atrial septal defect can cause the movement of oxygen-rich blood from the left atrium to the right. It puts a lot of strain on the right side of the heart as well as in the lungs.
If the hole is small, a baby or child with it will have no significant problems except murmurs in the heart. But if the hole is large, children with it may have symptoms of getting tired while playing, getting frequent cough/cold/chest infections and poor weight gain.
Causes of Atrial septal defect
An atrial septal defect is a developmental disorder present at birth. What exactly causes it is not very clear. There are certain factors affecting mothers during pregnancy that increase the risk of ASD and other heart defects in babies. Some of the known risk factors are family history of heart defects, mother on certain medications in early pregnancy, diabetes in mother from early pregnancy, IVF pregnancy, anomaly scan showing a defect in any other organ system of the fetus (brain, gut, kidney etc).
How blood flows in a heart with an ASD
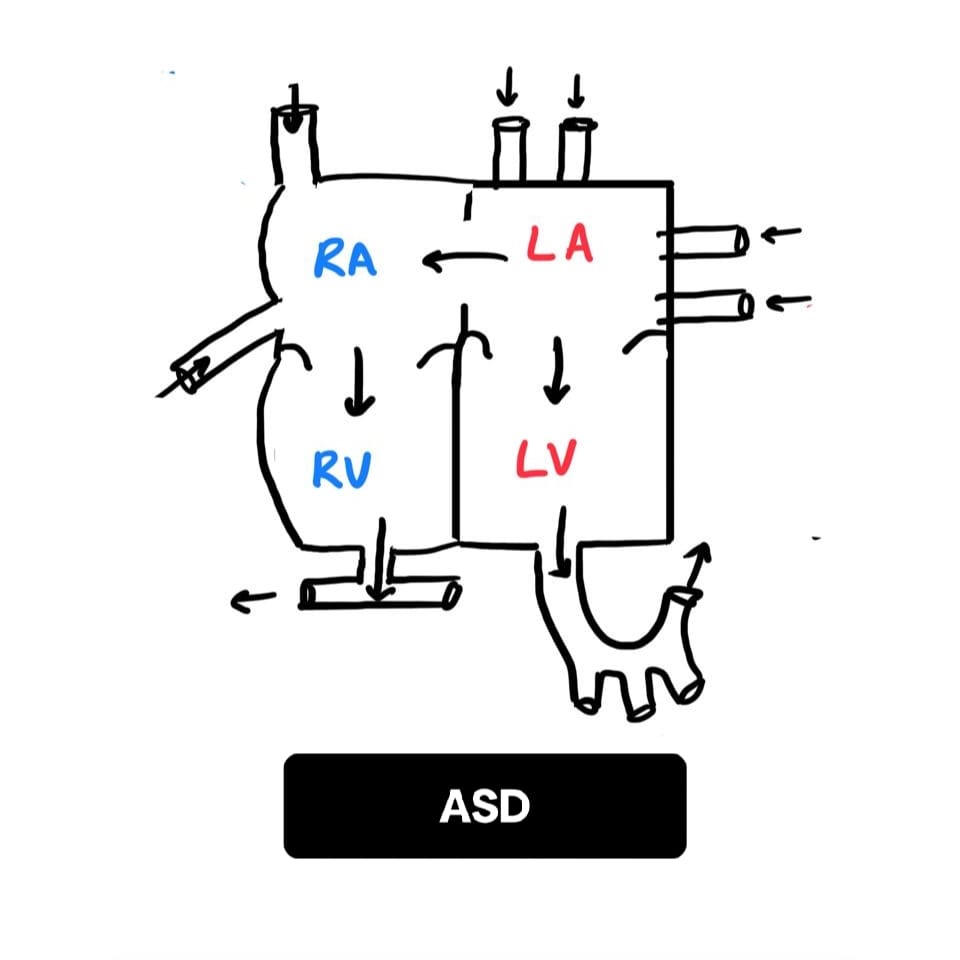
To understand ASD better, it is important to know how the normal heart works. The left heart has 2 chambers and the right heart has 2 chambers. The top 2 chambers (RA and LA) are the collecting chambers while the bottom 2 chambers (RV and LV) are pumping chambers. Pure blood is pumped by the LV to the whole body. The body’s organs uses the oxygen in that blood and makes the blood impure. The impure blood returns to the RA and is pumped by the RV to the lungs. When we breathe, the oxygen in our breath enters the blood and makes it pure again. The pure blood enters LA and is pumped out to the body by the LV.
Thus the heart supports 2 circuits. The left circuit pumps pure blood to the body and the right circuit pumps impure blood to the lungs. In a child with an ASD, the wall (SEPTUM) between the LA and the RA has a hole in it. So blood flows from the LA to the RA and then to the RV and the lungs. This means extra blood ends up going to the lungs. The congested lungs get infected relatively easily. Also, the RA and RV become bigger in size and pressure on that side of the heart also rises over time.
Complications of ASD
- Enlargement of the right side of the heart
- Right-sided heart failure
- High pressure of the right side of the heart (called pulmonary hypertension)
- Arrhythmias or abnormalities in heart rhythm
ASD types
There are four main types of ASD, according to the location of the defect in the septal wall.
- Secundum: This is the most common one, accounting for seventy percent of all ASDs. The hole is in the middle of the septum. A cardiac catheterization will help to close most secundum ASDs but a detailed echocardiogram and other technical factors only can tell if it is safe to close it by that method.
- Primum: Accounts for 20% of all ASDs. The defect is lower part of the septum. Other congenital heart defects may also be present along with this. This requires open-heart surgery for correction.
- Sinus venosus ASD: The defect occurs in the upper part of the septum and is associated with a wrong connection of right pulmonary vein to the LA.
ASD diagnosis
In a child with a doubt of an ASD, the doctor will advise the following diagnostic tests.
- Echocardiogram: this is sonography of the heart. It provides all required details about the ASD and its effect on the heart.
- ECG
- Cardiac catheterization
- CT scan
- Chest X-ray
ASD repair surgery – When to do
In a child with an ASD, a cardiologist will look into the following aspects:
- Age of the child
- The severity of symptoms
- Type and size of the ASD
- Effect on the heart
- Associated defects in the heart
It is important to get the ASD closed at the right time, before it affects the child too much or the changes in the heart become significant. The best time to close a simple typical ASD is at the age of 3-4 years. Sometimes, some ASDs need to be closed earlier.
Treatment for ASD
There are 2 methods to close an ASD.
- Open heart surgery: During an ASD repair surgery, the surgeon closes the defect with a patch. The surgeon may choose to close the hole by a cut made in the middle of the chest (sternotomy). In certain cases, the cut may be made on the right side of the chest; this is more cosmetic. A child having the surgery will have general anesthesia. So there will be no pain during surgery. The child will be in an Intensive care unit for a day after surgery and will go back to the room the next day. The average stay in the hospital will be for three to four days.
- Cardiac catheterization: An interventional cardiologist closes the hole by placing an umbrella device through groin vessels. No cuts or sutures are involved. The patient can go home the next day and takes aspirin (a mild blood thinner) for 6 months.
Only a pediatric cardiac specialist can determine which is the method best suited to close an ASD: surgery or device. Certain holes can only be closed by surgery while others can be closed by either method.
ASD FAQs
- What causes an atrial septal defect?
An atrial septal defect is a developmental disorder present at birth. Certain factors during pregnancy like maternal diabetes, medications, IVF, or other fetal anomalies can increase risk. - Is ASD life-threatening?
An ASD is not life-threatening. Most isolated ASDs can be closed in a planned manner. - Will an ASD come back after treatment?
No, both surgical and device-based closures are permanent, one-time procedures. - Which is the best age to do an ASD repair surgery?
Ideally between 3–4 years of age. In babies with complications like poor weight gain or recurrent infections, it may be done earlier. - What is the cost of ASD surgery in India?
It ranges from ---- to ----. International patients typically need to stay 10–14 days.
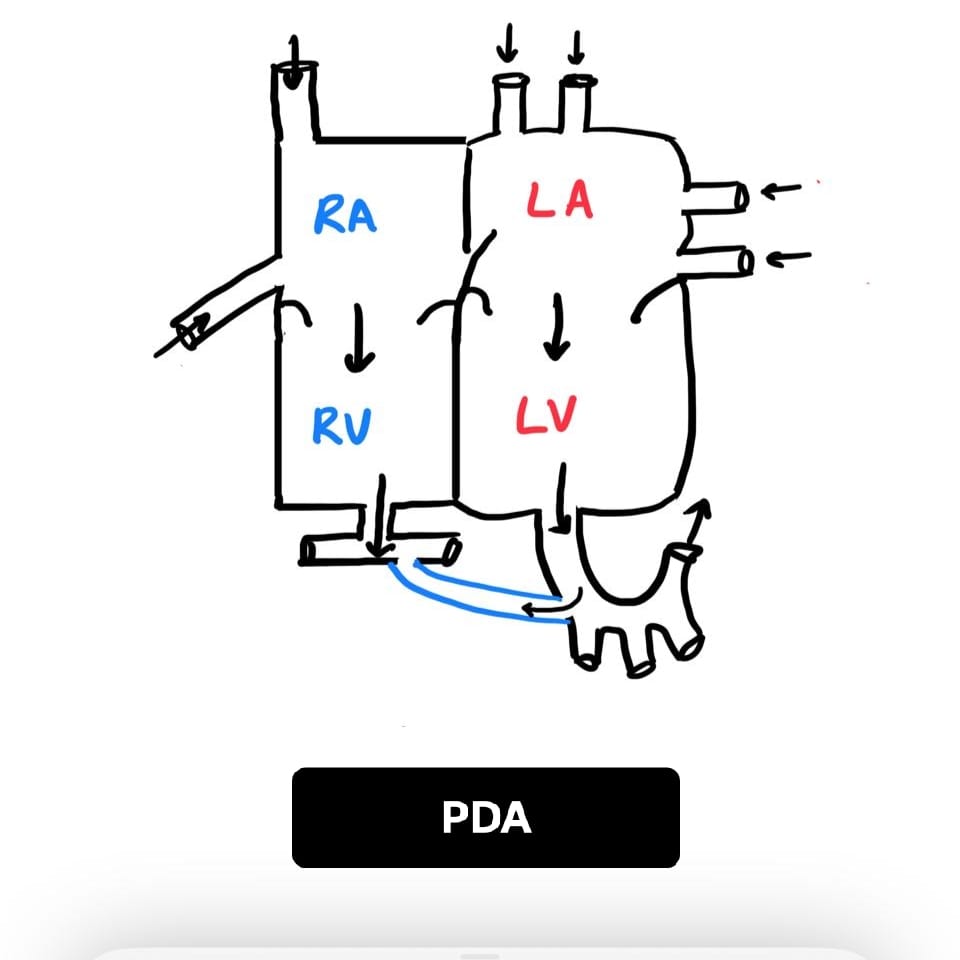
Patent Ductus Arteriosus (PDA)
A PDA is a blood vessel connection between the aorta and the pulmonary artery that should close after birth but remains open. When it stays open, extra blood keeps flowing between the lungs and the body circulation.
How blood flows in a PDA
In a PDA, blood can move between the aorta and pulmonary artery after birth. Depending on the size of the connection, the extra flow may cause faster breathing, poor feeding, recurrent chest infections, or a heart murmur.
Diagnosis of PDA
An echocardiogram is the main test. It shows the size of the duct and whether the PDA is putting strain on the heart or lungs. ECG and chest X-ray may also help.
Treatment of PDA
Small PDAs may close on their own or with medicines in selected babies. Larger PDAs are often closed by a catheter-based device, and some require surgery depending on size and anatomy.
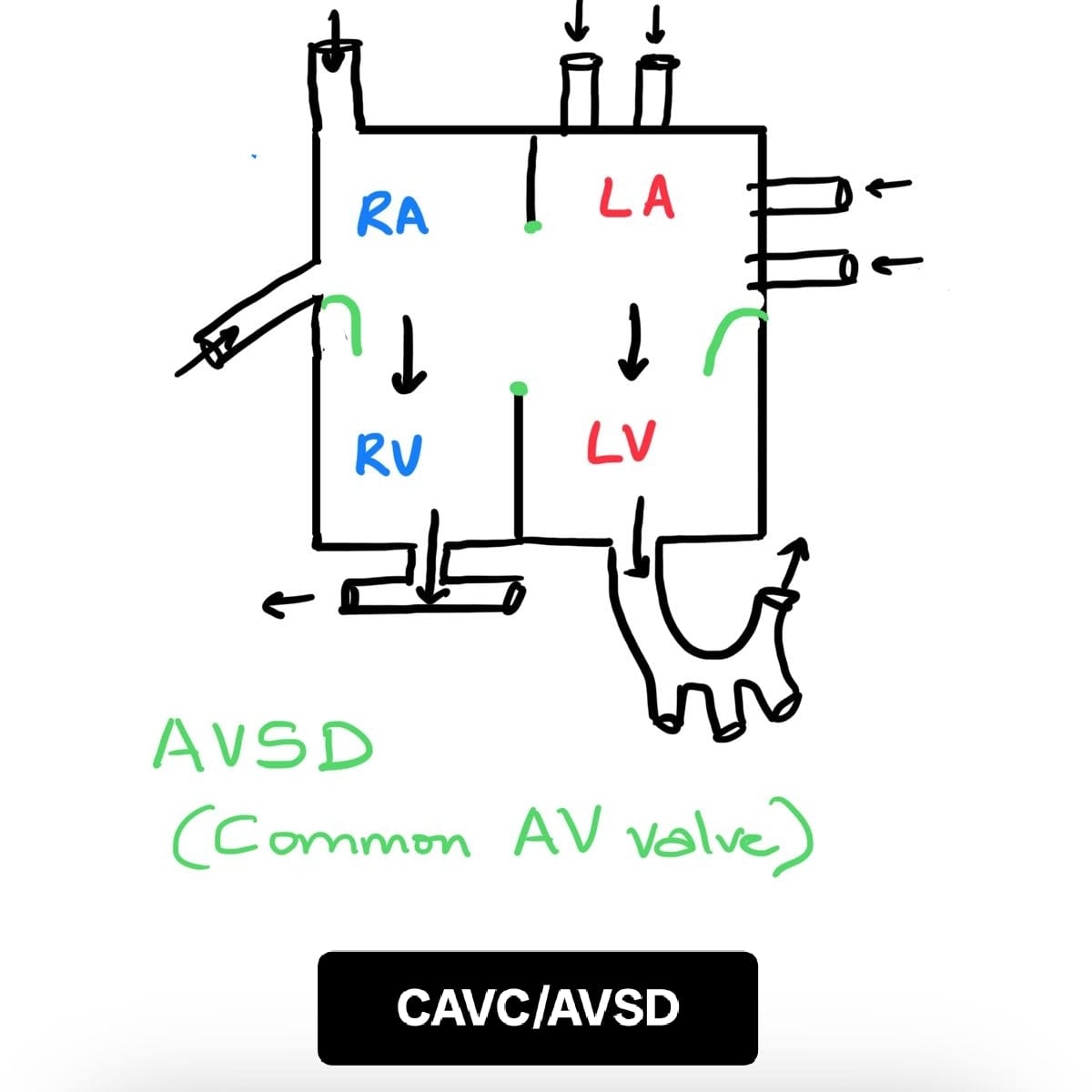
Atrioventricular Septal Defect (AVSD / CAVC)
An AVSD, also called a common atrioventricular canal defect or CAVC, means there is a common AV valve instead of separate mitral and tricuspid valves. It is often associated with holes between the upper and lower chambers of the heart.
Why AVSD matters
Because the valves and septa are not formed normally, blood can mix between the chambers and strain the lungs and the heart. The severity depends on the exact anatomy and whether there is a partial or complete AVSD.
Diagnosis of AVSD
Echocardiography is the key test. It shows the common valve, the size of any atrial or ventricular holes, and how the heart is functioning.
Treatment of AVSD
Most children with a complete AVSD need planned open-heart surgery in infancy or early childhood. The exact timing depends on symptoms, weight gain, and pressure changes in the lungs.
Truncus Arteriosus
Truncus arteriosus is a rare congenital heart defect.
It is a major heart defect and causes affected babies to breath faster, drink milk with difficulty and be prone to catch lung infections. The structure of the heart is altered such that instead of 2 major vessels coming out of the heart, there is just one which does the work of both vessels. There is also a hole in the heart.
Truncus arteriosus will need open heart surgery to repair. It is ideal to do the surgery before the baby is a month old. Undue delay in surgery can cause severe fatal complications.
Causes
Truncus Arteriosus (TA) is a developmental disorder present at birth. What exactly causes it is not very clear. There are certain factors affecting mothers during pregnancy that increase the risk of TA and other heart defects in babies. Some of the known risk factors are family history of heart defects, mother on certain medications in early pregnancy, diabetes in mother from early pregnancy, IVF pregnancy, anomaly scan showing a defect in any other organ system of the fetus (brain, gut, kidney etc), mother indulging in alcohol/smoking in early pregnancy, German measles, high fever in early pregnancy. Since the heart is formed in the first 2 months of pregnancy, it is then that the above factors play a role! Apart from these, babies with chromosomal disorders like DiGeorge syndrome and velocardiofacial syndrome are more at risk. Truncus arteriosus can also occur in babies without any of these risk factors.
How blood flows in a heart with Truncus Arteriosus
To understand TA better, it is important to know how the normal heart works. The left heart has 2 chambers and the right heart has 2 chambers. The top 2 chambers (RA and LA) are the collecting chambers while the bottom 2 chambers (RV and LV) are pumping chambers. Pure blood is pumped by the LV to the whole body through the AORTA. The body’s organs uses the oxygen in that blood and makes the blood impure. The impure blood returns to the RA and is pumped by the RV to the lungs through the PULMONARY ARTERY. When we breathe, the oxygen in our breath enters the blood and makes it pure again. The pure blood enters LA and is pumped out to the body by the LV.
Thus the heart supports 2 circuits. The left circuit pumps pure blood to the body and the right circuit pumps impure blood to the lungs. In a child with a TA, there are no separate AORTA or PULMONARY ARTERY. Instead, blood exits the LV and the RV through a vessel (called TRUNCUS) that continues as both the pulmonary artery AND the aorta! There is a large hole in the wall (SEPTUM) between the LV and the RV. So blood flows from the LV and RV to the TRUNCUS and then to the lungs AND to the body. Every part of the body receives a mixture of pure and impure blood. This also means extra blood ends up going to the lungs. The congested lungs get infected relatively easily. Also, the heart becomes bigger in size and pressure on the right side of the heart also rises over time.
Symptoms
- Breathing problems - fast and shallow
- Poor feeding - suck-rest-suck cycle
- Excessive sleepiness
- Pounding of heart and increased heart rate
- Bluish discoloration of the skin
- Poor growth and failure to thrive without timely treatment
Complications
- Severe breathing difficulty due to fluid in the lungs
- Persistent pulmonary hypertension
- Enlargement of the heart
- Heart failure due to worsening complications
Diagnosis of Truncus Arteriosus
- Echocardiogram: Ultrasound of the heart that gives structural details.
- Chest X-ray: Assesses lung status and fluid accumulation.
- CT scan: Used when pulmonary arteries aren’t clearly visible on echo.
- FISH test: Detects chromosome abnormalities like DiGeorge syndrome.
Types of Truncus Arteriosus
There are different types of TA based on anatomy of the Truncus. Some types (e.g. those with narrowed aorta) may require earlier surgery.
Truncus Arteriosus surgery – When to do?
Babies should ideally have surgery within the first month of life, and definitely before three months to avoid severe complications.
Surgery for Truncus Arteriosus
The surgery is open-heart under general anesthesia and involves several key steps:
- Separate the pulmonary artery from the aorta
- Connect the pulmonary artery to the RV using a conduit/tube
- Close the hole (VSD) between LV and RV
The procedure takes about 4–5 hours and is followed by care in the pediatric cardiac ICU. Tubes and wires will assist recovery and be removed gradually. Full recovery takes a few weeks, and hospital stay ends within days of ICU discharge.
Aftercare
Post-surgery, babies will grow normally and have no major activity restrictions. However, regular cardiac follow-up is necessary. As the child grows, the tube placed during surgery may need replacement with a larger one.
FAQs – Truncus Arteriosus
- What is truncus arteriosus?
In this defect, the aorta and pulmonary artery do not separate, resulting in a single vessel (truncus arteriosus). - Can truncus arteriosus be cured?
Yes, with early surgery in the first month, followed by possible re-interventions as the child grows. - Is truncus arteriosus life threatening?
Yes. Without surgery, infants may not survive beyond a few months. - How do you fix truncus arteriosus?
Close the VSD, create a pulmonary artery, and reconnect the aorta correctly via open-heart surgery.
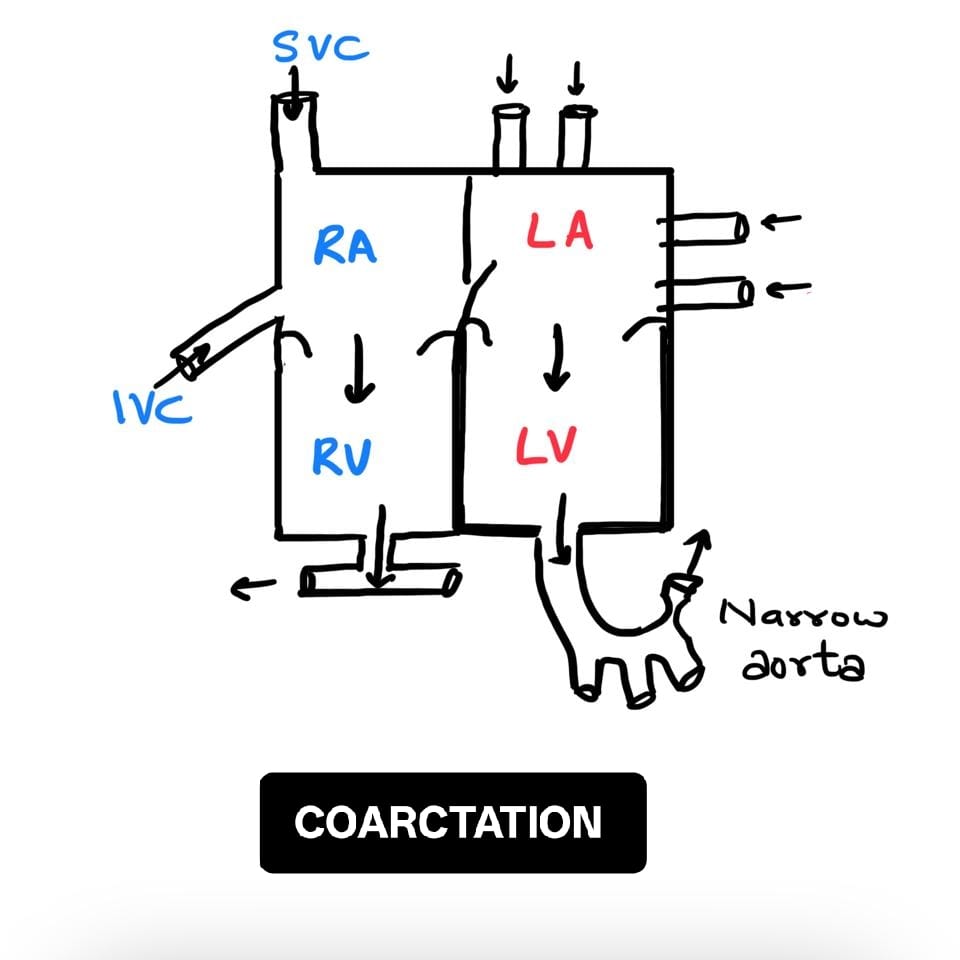
Coarctation of Aorta
Coarctation of the aorta is a heart defect present at birth. In this condition, there is a constriction or narrowing in the aorta, which is the main artery supplying blood to the entire body. It thus prevents the proper flow of blood from the heart to lower parts of the body as the narrowing is 99% of the time just after branches to the upper parts of the body are given off.
If the narrowing is severe, the heart will find it very tough to pump blood. It will also lead to heart failure later. Most of the babies with the problem will need emergency heart surgery or a balloon catheter procedure to repair the defect.
Causes
Coarctation is a developmental disorder present at birth. What exactly causes it is not very clear. There are certain factors affecting mothers during pregnancy that increase the risk of coarctation and other heart defects in babies. Some of the known risk factors are family history of heart defects, mother on certain medications or getting German measles in early pregnancy, diabetes in mother from early pregnancy, IVF pregnancy or anomaly scan showing a defect in any other organ system of the fetus (brain, gut, kidney etc). Coarctation is also more common in babies with Turners syndrome, a genetic disorder. Coarctation usually occurs close to the ductus arteriosus, which is an artery that is present only while a child is in the womb. After birth, this artery closes by itself. Scientists believe that coarctation may happen during this due to pinching of the walls of the aorta.
Signs and Symptoms
The symptoms usually depend on how severe the obstruction to blood flow through the aorta is. If there is severe narrowing, the symptoms will show at a very early stage, usually soon after birth. If the obstruction is mild, the symptoms will appear later in life.
- Pale skin
- Difficulty in breathing or fast breathing
- Profuse sweating
- Severe irritability
- Difficulty in feeding
- Lethargy
- High blood pressure in the arms and low BP in the legs
- Headaches
- Pain in the legs after playing
- Fatigue
Very often, children will not have any clear signs or symptoms except for high blood pressure. Hence it is recommended that a child’s BP be checked at every well child visit to the pediatrician after age of 3 years.
Complications of Coarctation
- Enlargement of the heart and weakening
- Threat to life as blood supply to the body is compromised and acid level in the blood increases
- High blood pressure in the upper part of the body and head
Diagnosis of Coarctation
- Echocardiogram: Provides a clear image of the structure of the heart and vessels
- ECG
- Chest X-ray
- CT or MRI scans of the heart
Treatment of Coarctation
Different approaches exist depending on age and severity:
- Newborns and infants: Surgery is preferred
- Older infants or children: Balloon angioplasty if the upper part of the aorta is normal; surgery if it is narrow
- Older children: Balloon angioplasty or stent placement
Surgery Options:
- Resection with end-to-end anastomosis: Remove narrow portion and reconnect ends
- Subclavian aortoplasty: Use part of subclavian artery to repair coarctation
- Patch aortoplasty: Add synthetic patch to the cut ends
- Tubular bypass graft: Bypass narrow area with graft
Balloon Angioplasty: A catheter with balloon tip is guided to coarctation and inflated to widen the area. May be repeated.
Stenting: A metal mesh stent is placed and expanded to keep the narrowed section open. It can be dilated over time but not ideal for small children.
Aftercare
Regular check-ups are essential in the pediatric cardiac OPD. No diet or activity restrictions. Special tests may be needed as the child grows.
FAQs – Coarctation of Aorta
- What causes coarctation of the aorta?
Coarctation is a congenital heart defect where there is a narrowing of the aorta at a particular point. Exact cause is unknown. - Can coarctation of the aorta be cured?
Yes. Surgery or balloon-stent procedures can provide full recovery and good quality of life. Lifelong follow-up is needed. - Can coarctation of aorta be detected before birth?
Severe coarctation can be detected on fetal echocardiogram. In most cases, the report may say "strongly suspicious of coarctation".
Single Ventricle Defect
Heart defects in children are of many types. Amongst the complex ones, the single ventricles are common. In these kind of heart defects, the heart is malformed such that there is mixing of pure and impure blood inside the heart and the same blood is pumped to the whole body. In addition, the flow to the lungs may be less or much more than normal.
Symptoms that a baby/child with a single ventricle has (will not have all of the symptoms below but a combination of them):
- Failure to gain weight or slow weight gain
- Blue lips, palms and soles that may become more blue with cold exposure or with crying
- Repeated cough/cold/pneumonia
- Getting tired with mild activities, gets tired sooner than playmates
Normal heart vs single ventricle
To understand the single ventricle better, it is important to know how the normal heart works. The left heart has 2 chambers and the right heart has 2 chambers. The top 2 chambers (RA and LA) are the collecting chambers while the bottom 2 chambers (RV and LV) are pumping chambers. Pure blood is pumped by the LV to the whole body. The body’s organs uses the oxygen in that blood and makes the blood impure. The impure blood returns to the RA and is pumped by the RV to the lungs. When we breathe, the oxygen in our breath enters the blood and makes it pure again. The pure blood enters LA and is pumped out to the body by the LV. Thus the heart supports 2 circuits. The left circuit pumps pure blood to the body and the right circuit pumps impure blood to the lungs.
What is a Fontan surgery?
In single ventricles, the heart malformation is so severe that the pediatric cardiac surgeon cannot separate out the 2 circuits. Instead, for the past 50 years, they have been bypassing the heart to send blood to the lungs directly. This serves 2 purposes, the impure blood no longer enters the heart and only the pure blood is pumped out to the body. This kind of surgery is called Fontan surgery, after Dr Fontan who first performed it, in 1971. Most often, the surgery is done in 2 stages. The first stage is called Glenn surgery and the second stage is called Fontan surgery. There is a separation of atleast 1 year between the 2 surgeries, in most instances.
Types of single ventricles:
- Tricuspid atresia
- Mitral atresia
- Aortic atresia
- Double Inlet Left Ventricle
- Pulmonary atresia with hypoplastic RV
- Double outlet RV (DORV) with hypoplastic LV or RV
- DORV with remote vsd
- Common AV valve with hypoplastic LV or RV
Diagnosis of Single Ventricle
- The echocardiogram is the best test to diagnose single ventricle and is essential.
- An electrocardiogram (ECG) is important to study the heart rate and rhythm.
- The pulse oximeter gives the oxygen saturation of the blood circulating in the body.
- Rarely, a CT scan of the chest is required to study minute details of the heart vessels.
- A cardiac catheterization may also be required in some cases.
Glenn surgery:
The impure blood from the upper part of the body returns to the heart via a vein called the SVC. In the Glenn surgery, the SVC is disconnected from the heart and connected to the lung arteries.
Glenn surgery can be performed at any age, earliest being 2-3 months. The ideal age of performing Glenn surgery is 6-12 months of age.
After Glenn surgery, the child is expected to be less blue and be able to exert better.
Fontan surgery:
The impure blood from the lower part of the body returns to the heart via a vein called the IVC. In the Fontan surgery, the IVC is disconnected from the heart and connected to the lung arteries by using a tube.
Fontan surgery can be performed earliest at age 4-5 years or weight of 15kg.
After the Fontan surgery, the child is expected to have complete separation of impure and pure blood and hence have a normal colour and be able to exert normally.
Post operative stay
A pediatric cardiac surgeon does the Glenn/Fontan surgeries. The duration of the operation for Glenn is 3-4 hours and for Fontan is longer as the earlier Glenn surgery causes the chest to have scar tissue surrounding the heart. Your child will stay in the hospital for 10-12 days after the surgery.
If not treated, the child with the single ventricle will not thrive. He/she will not be able to grow properly and even routine activities may become difficult for them.
Risk and Complication of Glenn and Fontan Surgery
The rate of complications after Glenn and Fontan surgery depends a lot on the status of the child’s lung arteries and also certain pressure numbers of the heart and vessels. These factors are not in control of the operating team. In general, the most common complication is the need for chest tubes to be in place for many days, rarely weeks.
There are some long term complications of the Fontan surgery: heart failure, protein losing enteropathy, plastic bronchitis and liver disease are some of the top concerns. These may manifest years later. A lot of new medicines are available to control the complications. If everything fails, then heart transplantation is an option.
FAQs – Single Ventricle
- What does a single ventricle mean?
Your heart has two ventricles, the right ventricle, and the left ventricle. These ventricles pump blood from the heart to the body. Our heart needs both of these to function correctly. A single ventricle defect is when you have only one ventricle that works. It is a serious heart defect that requires surgery. - Can you live with one ventricle?
The right and left ventricles in our heart pump the blood out to the body. You need both these for our heart to work correctly. If there is only one ventricle, the baby will not survive for long without a surgery. - What is a Fontan procedure for the heart?
Fontan surgery is the right surgical option for single ventricle defect. This is the name given to the last surgery done for a child with a single ventricle defect. The remaining source of blue blood returning to the heart (the IVC) is disconnected from the heart and instead connected to the pulmonary (lung arteries). - What is the right age for Glenn and Fontan surgeries?
The right age for Glenn surgery is between 6-12 months of birth. The earliest time is after 2 months of birth. Fontan surgery is usually done when the baby is between 4-5 years of age and the body weight is around 15 Kilograms. - How is life for the child after Fontan surgery?
Life after Fontan surgery is a big change for the child. He or she no longer gets tired after walking/running. In fact, exercises, especially of the lower legs (running, biking, swimming) and breathing exercises are encouraged in the child after surgery. The child is able to resume normal routine after a month. Going to school, participating in non competitive sports and also household chores is permitted. Medications to be taken are minimum. There is no restriction on diet either. The child with Fontan operation will need life long follow up. Periodic visits to the pediatric cardiac OPD will ensure that complications if any are picked up before they cause trouble to the child. Such visits are also occasions to discuss the road ahead at different stages of life (puberty, becoming financially independent, pregnancy etc).
D-Transposition of the Great Arteries (DTGA)
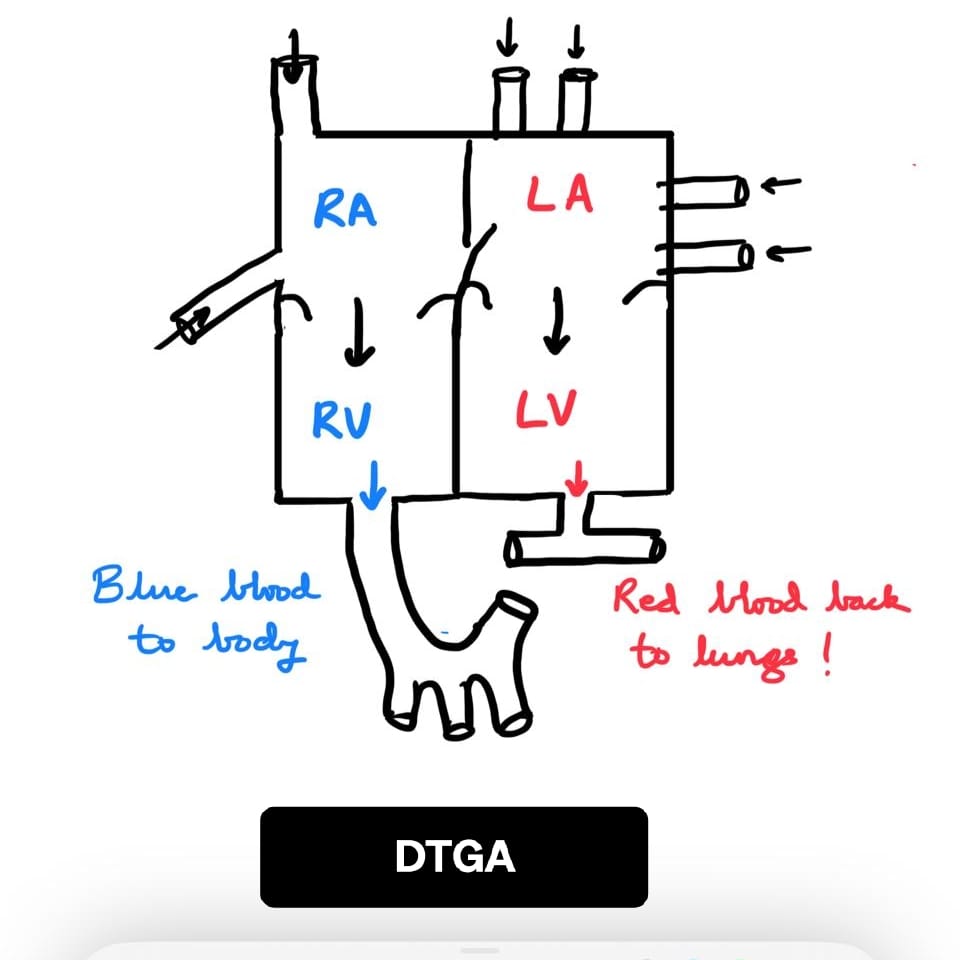
D-Transposition of the Great Arteries (DTGA) is a serious congenital heart defect, meaning it is present at birth. In this condition, the two major arteries that carry blood away from the heart—the pulmonary artery and the aorta—are switched (transposed) from their normal positions. This results in a situation where oxygen-rich blood from the lungs goes back to the lungs, and oxygen-poor blood from the body goes back to the body, without proper mixing. Without treatment, this condition is life-threatening.
Why did my baby get DTGA?
We understand that parents naturally want to know why this happened. Unfortunately, in most cases, there is no clear or single cause. DTGA is a developmental disorder—it occurs while the baby’s heart is forming in the womb.
Some factors known to increase the risk of DTGA and other congenital heart defects include:
- A family history of heart defects
- The mother taking certain medications in early pregnancy
- Diabetes in the mother from early pregnancy
- IVF (in-vitro fertilization) pregnancy
- Anomaly scans showing defects in other organs (brain, kidneys, gut, etc.)
- In a small percentage of cases, chromosomal abnormalities may be found in the baby
Even with all we know, many babies with DTGA are born to perfectly healthy mothers with no identifiable risk factors. It is important to remember: this is not your fault.
What is the actual defect in DTGA?
In a normal heart:
- The right ventricle pumps oxygen-poor (blue) blood into the lungs via the pulmonary artery
- The left ventricle pumps oxygen-rich (red) blood to the body via the aorta
In DTGA:
- The aorta arises from the right ventricle, carrying oxygen-poor, blue blood to the whole body
- The pulmonary artery arises from the left ventricle, sending oxygen-rich red blood back to the lungs
Because of this incorrect connection, the two blood circuits do not mix, and the body doesn't receive the oxygen it needs, hence the baby is blue.
How blood flows in a heart with DTGA
In a newborn with DTGA:
- Blood from the body returns to the right heart, and is pumped straight back to the body without picking up oxygen
- Blood from the lungs returns to the left heart, and is pumped straight back to the lungs
This results in two separate, non-communicating circuits. For survival, there must be some mixing of blood, which can occur through:
- A hole between the atria (atrial septal defect or patent foramen ovale)
- A hole between the ventricles (ventricular septal defect)
- A connection between the aorta and pulmonary artery (ductus arteriosus)
These natural or temporary connections are critical in the early days after birth.
Effect of DTGA on the Baby
Babies with DTGA usually appear blue (cyanotic) shortly after birth because of low oxygen levels. Other signs may include:
- Rapid breathing
- Poor feeding
- Lethargy
- Low oxygen saturation despite breathing room air
If not promptly treated, low oxygen levels can lead to serious complications affecting the brain and other organs.
How is DTGA diagnosed?
In many cases, DTGA is suspected soon after birth based on the baby's bluish color and low oxygen levels. A pediatric cardiologist confirms the diagnosis using:
- Echocardiography (heart ultrasound) – This is the most important test to visualize the heart anatomy and function
- Pulse oximetry – To measure oxygen saturation
- Sometimes, DTGA is picked up before birth during a fetal echocardiogram, especially in high-risk pregnancies
How is DTGA treated?
DTGA requires surgical correction soon after birth. The treatment may involve:
-
Stabilization
- A medicine called Prostaglandin E1 is given to keep the ductus arteriosus open, allowing some mixing of blood.
- Sometimes, a bedside procedure called a balloon atrial septostomy is done to enlarge the hole between the atria and improve mixing.
-
Surgical Repair: Arterial Switch Operation (ASO)
- This is the definitive treatment and is usually performed within the first 1–2 weeks of life.
- The surgeon switches the aorta and pulmonary artery back to their correct positions, and the coronary arteries (which supply the heart itself) are reimplanted.
- The heart is then able to circulate oxygen-rich blood to the body normally.
What is the outlook after surgery?
The outlook for babies with DTGA has dramatically improved over the years. With successful surgery:
- Most children grow and develop normally
- Regular follow-up with a pediatric cardiologist is essential
- Some children may need medications or minor interventions later, but major complications are uncommon
- Physical activity is usually well-tolerated, though each child is assessed individually
Long-term follow-up includes:
- Monitoring heart function and rhythm
- Watching for narrowing of arteries or valve-related issues
- Support for neurodevelopment, especially in babies who had complications before surgery
Final Thoughts
As pediatric cardiologists, we understand the shock and anxiety of receiving a diagnosis like DTGA. But with early diagnosis, skilled surgery, and dedicated follow-up care, your baby can go on to live a full and active life.
Please don’t hesitate to reach out with your questions or concerns—we’re here for you every step of the way.
Pediatric Heart Transplant
A pediatric heart transplant is a life-saving surgery in which a child with severe heart disease (that doesn't respond to medicines anymore) receives a healthy heart from a donor. This new heart takes over the function of pumping blood through the body. While the idea of a transplant may sound overwhelming, it offers many children a chance at a longer, healthier life.
Who Needs a Pediatric Heart Transplant?
Children may need a heart transplant for various reasons. The 2 most common include cardiomyopathies (Eg. DCM, RCM), congenital heart defects where surgery cannot be done or has failed.
Who is a Heart Donor?
A heart donor is usually a child or young adult who has suffered brain death, meaning their brain has irreversibly stopped working, but their other organs—including the heart—are still healthy. The family of the donor makes the generous and brave decision to donate the child’s organs so that other children may live. Donor hearts come from across the country and are matched through an organ sharing network, which is a government body.
How is a Donor Heart Matched to a Child?
Matching a donor heart to a recipient child is a careful process. Doctors look at blood group compatibility, body size, and urgency of the child’s condition. In some cases, additional tests are done to check for antibodies in the child’s blood that could react against the donor organ. Once a suitable donor is found, the transplant surgery is performed as quickly as possible—often within hours—because a heart remains viable outside the body only for a short time.
The Heart Transplant Process in Brief
Once a child is listed for transplant, they are closely monitored by their medical team. When a donor heart becomes available, the child is immediately admitted for surgery. The transplant operation is carried out by a skilled team of pediatric cardiac surgeons, anesthetists, and nurses. After surgery, the child stays in the intensive care unit (ICU) for a few days, followed by a longer stay in the hospital for recovery and monitoring. The child will need regular follow-ups, tests, and lifelong medication to prevent the body from rejecting the new heart. Medicines cannot be missed for even one day. So, getting a new heart is NOT quite like a car getting a new engine ...
Life After a Heart Transplant
Many children go on to live active and fulfilling lives after a heart transplant. With good care and family support, children can return to school, participate in most activities, and enjoy a good quality of life. At each follow up visit in the OPD, the doctor will check for general well being, rejection of the heart and side effects of the daily medications.
The Importance of Organ Donation
Pediatric heart transplantation is only possible because of the incredible gift of organ donation. In India, the field of organ transplantation is growing rapidly, and we are poised to become one of the leading countries in heart transplant numbers. But many children still wait for a donor heart. By choosing to donate organs, families can turn tragedy into hope for others.
If you would like to know more about organ donation or how to register as a donor, please call India’s national 24-hour free organ donation helpline at 1800 11 4770. Every donor is a hero.
Fetal Echo
All about detecting heart defects in the baby before they are born. The heart of the baby is formed in the first 2 months of pregnancy. This is the time when the lady realizes she is pregnant, and the heart is already formed then! At 2 months, the heart of the baby (called FETUS) is too small to be examined by ultrasonography. At the end of 3 months (11-13 weeks), the sonographer may get some clue about whether a heart defect is present. The heart of the fetus can be better examined at 4-5 months of gestation (18-22 weeks).
What is a fetal echocardiogram (fetal echo)?
A fetal echo is an ultrasound of the fetus’s heart done by specially trained pediatric cardiologists or sonologists. The focus is on a detailed view of the fetal heart. Pediatric cardiologists are able to then guide and counsel the family about any abnormal findings. It is best done at 18-22 weeks of pregnancy.
What are the reasons a FETAL ECHO should be done for your baby?
A doctor will order it if there are certain indications like:
- 11-13 week scan positive for increased NT or tricuspid regurgitation or flow reversal in the ductus venosus.
- Suspected major anomaly in any organ system in the anomaly scan
- Fetal arrhythmias
- Hydrops fetalis/ monochorionic twin pregnancy.
- Intracardiac echogenic focus IF there are other associated soft markers for aneuploidy
- Fetal Chromosomal abnormalities
- Pre gestational maternal diabetes
- IVF pregnancy
- Family history of congenital heart disease
- Maternal autoimmune disease
- Mother taking certain medications (e.g., retinoids)
- Mother had infection(high fever, TORCH) in first trimester
Can fetal echo pick up all heart defects?
- Can pick up most major heart defects like TOF, DORV, TGA, Single Ventricles, AV septal defects
- Fetal echo can miss coarctation of the aorta and tapvc many times. It can also miss VSDs
Prenatal cardiac counselling
Prenatal counselling by a pediatric cardiac specialist may help prepare the family mentally and financially for what to expect after birth. Counselling can also help in allaying anxiety in isolated fetal findings like ARSCA, LSVC, vsd, right aortic arch etc.
Recurrence of CHD in next pregnancy
There is a high chance of the next pregnancy being normal. However, the odds are not the same as the general population. For example, if there is coarctation in the fetus, the chance that the next fetus will have some kind of left heart obstructive lesion is higher than the general population but remains low overall.
Pulse Oximetry Screening
The American Academy of Pediatrics (AAP) recommends checking the pulse oximetry reading (saturation) of every newborn after 24 hours of birth (or better still, at time of discharge home, if later than 24 hours old). This test is a “Fail” if the saturation is less than 94%. This simple screening test can pick up major cyanotic CHD. This should be implemented in Maharashtra as well.
References
- American Institute of Ultrasound in Medicine/American Society of Echocardiography/Fetal Heart Society. 2023 Guidelines for performance of the Fetal Echocardiogram: An update.